![]()
|
|
| Re: Big Minnesota health insurer, PreferredOne, departs ACA website citing cost of doing business (1106303) | |
|
|
|
| Home > OTChat | |
[ Post a New Response | Return to the Index ]
|
Page 23 of 25 |
||
| (1226513) | |
Re: Big Minnesota health insurer, PreferredOne, departs ACA website citing cost of doing business |
|
|
Posted by 3-9 on Tue Sep 16 19:28:28 2014, in response to Big Minnesota health insurer, PreferredOne, departs ACA website citing cost of doing business, posted by Olog-hai on Tue Sep 16 18:33:50 2014. There's something fishy about it. Almost like, they have the lion's share of enrollees, so they have no need to stay on the exchange. And after they leave the exchange, they'll jack up the rates because the people won't take the trouble to compare with the exchange's plans without the easier comparison mechanism. |
|
| (1226526) | |
Re: Big Minnesota health insurer, PreferredOne, departs ACA website citing cost of doing business |
|
|
Posted by SelkirkTMO on Tue Sep 16 19:42:25 2014, in response to Re: Big Minnesota health insurer, PreferredOne, departs ACA website citing cost of doing business, posted by 3-9 on Tue Sep 16 19:28:28 2014. That's what made United Hellcare the megalith it is today. :) |
|
| (1227354) | |
Ezekiel Emanuel (ACA ''architect'') wants to die at 75 |
|
|
Posted by Olog-hai on Thu Sep 18 21:57:08 2014, in response to Ezekiel Emanuel (ACA "architect"): Vast majority of employers will drop healthcare coverage, posted by Olog-hai on Fri Mar 21 12:25:08 2014. Seems like he's trying to talk the rest of us into feeling that way too. (He's currently 57.)The Atlantic
|
|
| (1227357) | |
Re: Ezekiel Emanuel (ACA ''architect'') wants to die at 75 |
|
|
Posted by chicagomotorman on Thu Sep 18 22:02:42 2014, in response to Ezekiel Emanuel (ACA ''architect'') wants to die at 75, posted by Olog-hai on Thu Sep 18 21:57:08 2014. There will be warm place waiting for that evil self hating Jewish family. |
|
| (1227465) | |
Re: Ezekiel Emanuel (ACA ''architect'') wants to die at 75 |
|
|
Posted by FYBklyn1959 on Fri Sep 19 09:42:20 2014, in response to Ezekiel Emanuel (ACA ''architect'') wants to die at 75, posted by Olog-hai on Thu Sep 18 21:57:08 2014. I wonder if he is related to ScrabbleSHIT |
|
| (1227525) | |
Re: Ezekiel Emanuel (ACA ''architect'') wants to die at 75 |
|
|
Posted by Olog-hai on Fri Sep 19 12:30:38 2014, in response to Re: Ezekiel Emanuel (ACA ''architect'') wants to die at 75, posted by FYBklyn1959 on Fri Sep 19 09:42:20 2014. Good question. He's not as nihilistic, although he is nihilistic. |
|
| (1227539) | |
Re: Ezekiel Emanuel (ACA ''architect'') wants to die at 75 |
|
|
Posted by FYBklyn1959 on Fri Sep 19 12:46:51 2014, in response to Re: Ezekiel Emanuel (ACA ''architect'') wants to die at 75, posted by Olog-hai on Fri Sep 19 12:30:38 2014. Albeit, I don't think that Scrabble even wanted to live anywhere near 75 years (and since he hasn't posted in awhile, maybe he got his wish) :\ |
|
| (1231384) | |
Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer |
|
|
Posted by Olog-hai on Sun Oct 5 13:29:41 2014, in response to Universal Health Care is HERE in these USA! Apply Now. www.healthcare.gov, posted by SMAZ on Tue Oct 1 13:19:06 2013. Never mind more mendacity about the rate that premiums are increasing.Mediaite
|
|
| (1231423) | |
Re: Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer |
|
|
Posted by Nilet on Sun Oct 5 15:34:31 2014, in response to Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer, posted by Olog-hai on Sun Oct 5 13:29:41 2014. This is why private companies shouldn't be allowed anywhere near health care. |
|
| (1231438) | |
Re: Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a true answer |
|
|
Posted by italianstallion on Sun Oct 5 17:06:20 2014, in response to Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer, posted by Olog-hai on Sun Oct 5 13:29:41 2014. Not a smart-aleck answer, just a true one. You've got to shop around for a good deal. |
|
| (1231440) | |
Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer |
|
|
Posted by Olog-hai on Sun Oct 5 17:10:42 2014, in response to Re: Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a true answer, posted by italianstallion on Sun Oct 5 17:06:20 2014. Never mind an insulting answer. The fellow who lied about "if you like your plan/doctor" and who can't get it together with respect to the website is going to say that someone doesn't know how to shop around, never mind why he has to shop around?The devil has too many advocates. Knock it off before it hurts you. |
|
| (1231454) | |
Re: Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer |
|
|
Posted by italianstallion on Sun Oct 5 17:48:42 2014, in response to Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer, posted by Olog-hai on Sun Oct 5 17:10:42 2014. Website? Website is just fine, thank you. Another GOP false talking point. |
|
| (1231613) | |
Re: Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer |
|
|
Posted by RockParkMan on Mon Oct 6 07:33:54 2014, in response to Re: Indiana: Steel plant manager asks Obama why healthcare costs are rising, gets a smart-aleck answer, posted by italianstallion on Sun Oct 5 17:48:42 2014. Nazi chicken hawks have nothing but lies, |
|
| (1232073) | |
ACA website www.healthcare.gov still suffering from lack of transparency |
|
|
Posted by Olog-hai on Tue Oct 7 12:35:05 2014, in response to Universal Health Care is HERE in these USA! Apply Now. www.healthcare.gov, posted by SMAZ on Tue Oct 1 13:19:06 2013. NY Times
|
|
| (1233171) | |
Covered California awarding no-bid contracts in contravention of state oversight law |
|
|
Posted by Olog-hai on Sun Oct 12 14:04:31 2014, in response to Universal Health Care is HERE in these USA! Apply Now. www.healthcare.gov, posted by SMAZ on Tue Oct 1 13:19:06 2013. Associated Press
|
|
| (1237317) | |
House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by Olog-hai on Wed Oct 29 17:20:05 2014, in response to Universal Health Care is HERE in these USA! Apply Now. www.healthcare.gov, posted by SMAZ on Tue Oct 1 13:19:06 2013. Daily Therion
|
|
| (1237318) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by italianstallion on Wed Oct 29 17:24:18 2014, in response to House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by Olog-hai on Wed Oct 29 17:20:05 2014. Boy you are busy, busy, busy today. |
|
| (1237319) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by SelkirkTMO on Wed Oct 29 17:32:13 2014, in response to Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by italianstallion on Wed Oct 29 17:24:18 2014. Yeah, he's in a self-imposed Ebola quarantine in his basement. Mom is slipping snacks under the door though. :) |
|
| (1237323) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by italianstallion on Wed Oct 29 18:09:21 2014, in response to Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by SelkirkTMO on Wed Oct 29 17:32:13 2014. Ha! |
|
| (1237327) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by AlM on Wed Oct 29 18:26:10 2014, in response to House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by Olog-hai on Wed Oct 29 17:20:05 2014. So is the House introducing a technical corrections amendment to ACA to end this loophole? |
|
| (1237328) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by 3-9 on Wed Oct 29 18:30:02 2014, in response to House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by Olog-hai on Wed Oct 29 17:20:05 2014. They must be very poorly paid diplomats to qualify for all those subsidies. |
|
| (1237329) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by SelkirkTMO on Wed Oct 29 18:33:39 2014, in response to Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by AlM on Wed Oct 29 18:26:10 2014. Heh. :) |
|
| (1237332) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by Fred G on Wed Oct 29 18:40:25 2014, in response to Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by AlM on Wed Oct 29 18:26:10 2014. I would think so, for something this serious.your pal, Fred |
|
| (1237413) | |
Re: House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies |
|
|
Posted by bingbong on Thu Oct 30 02:02:35 2014, in response to House committees investigate IRS over why foreign diplomats are eligible for ACA subsidies, posted by Olog-hai on Wed Oct 29 17:20:05 2014. Criticism is ridiculous. Diplomatic staff residing in this country should be ale to access legal benefits of being here as they are here legally. |
|
| (1239751) | |
ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by Olog-hai on Mon Nov 10 11:48:38 2014, in response to Universal Health Care is HERE in these USA! Apply Now. www.healthcare.gov, posted by SMAZ on Tue Oct 1 13:19:06 2013.
|
|
| (1239752) | |
Re: ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by mtk52983 on Mon Nov 10 11:52:57 2014, in response to ACA architect admits no transparency in law, shows contempt for US voters, posted by Olog-hai on Mon Nov 10 11:48:38 2014. Are you telling me that people do not know that with any form of insurance that some people pay more in premiums than they actually use, some pay less and that the premiums are set up based on what insurance companies figure they will need to save from those who do not use it to cover those that do |
|
| (1239762) | |
Re: ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by Train Dude on Mon Nov 10 13:49:35 2014, in response to ACA architect admits no transparency in law, shows contempt for US voters, posted by Olog-hai on Mon Nov 10 11:48:38 2014. The law now faces its first serious challenge in the Supreme Court over the issue of subsidies. As written, this very poorly crafted law allows federal subsidies for states that established exchanges. Only 18 states did - technically making federal subsidies in 32 states illegal. If the subsidies are declared illegal, the collapse of the ACA will resemble the collapse of the World Trade Center. Look out below. |
|
| (1239802) | |
Re: ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by Olog-hai on Mon Nov 10 20:43:54 2014, in response to Re: ACA architect admits no transparency in law, shows contempt for US voters, posted by Train Dude on Mon Nov 10 13:49:35 2014. I wonder how John Roberts is feeling after he basically declared it a tax, but the whole DC establishment is upholding this "law" even though Herr Jonathan Gruber herein admits that it's a killer of the law?So much for the CBO. |
|
| (1239828) | |
Re: ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by train dude on Tue Nov 11 00:15:35 2014, in response to Re: ACA architect admits no transparency in law, shows contempt for US voters, posted by Olog-hai on Mon Nov 10 20:43:54 2014. Given the ambiguity of the section on subsidies, the Supremes will likely have to deem the subsidies unconstitutional. With the subsidies gone, ACA folds like a cheap card table. |
|
| (1239831) | |
Re: ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by Olog-hai on Tue Nov 11 01:01:19 2014, in response to Re: ACA architect admits no transparency in law, shows contempt for US voters, posted by train dude on Tue Nov 11 00:15:35 2014. Yeah . . . makes one wonder if that is the "beneficial crisis" that ought not go to waste in order to push single-payer deathcare. |
|
| (1239840) | |
Re: ACA architect admits no transparency in law, shows contempt for US voters |
|
|
Posted by Fred G on Tue Nov 11 04:26:02 2014, in response to ACA architect admits no transparency in law, shows contempt for US voters, posted by Olog-hai on Mon Nov 10 11:48:38 2014. So what kind of health insurance doesn't have healthy people pay in and doesn't have sick people getting paid?Your pal, Fred |
|
| (1240045) | |
ACA architect claims "regret" for contempt for US voters, does not deny no transparency in law |
|
|
Posted by Olog-hai on Wed Nov 12 10:58:51 2014, in response to ACA architect admits no transparency in law, shows contempt for US voters, posted by Olog-hai on Mon Nov 10 11:48:38 2014. "Regret" is not an apology. He only feels bad being caught expressing his true feelings, but has not changed his mind.Mediaite
|
|
| (1241328) | |
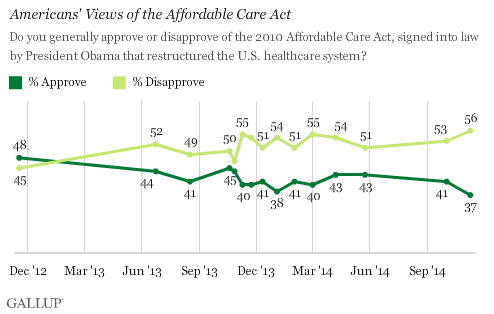
ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Olog-hai on Tue Nov 18 20:41:45 2014, in response to Universal Health Care is HERE in these USA! Apply Now. www.healthcare.gov, posted by SMAZ on Tue Oct 1 13:19:06 2013. Gallup
|
|
| (1241343) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by italianstallion on Tue Nov 18 23:28:37 2014, in response to ACA approval at 37 percent as new enrollment period commences, posted by Olog-hai on Tue Nov 18 20:41:45 2014. No surprise, in the face of constant false attacks on the law from Day 1. |
|
| (1241344) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Train Dude on Wed Nov 19 00:03:49 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by italianstallion on Tue Nov 18 23:28:37 2014. Or maybe the American public just resents being lied to. |
|
| (1241346) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Fred G on Wed Nov 19 00:15:51 2014, in response to ACA approval at 37 percent as new enrollment period commences, posted by Olog-hai on Tue Nov 18 20:41:45 2014. Yeahbut 70% of those insured are satisfied with their health care.your pal, Fred |
|
| (1241349) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Train Dude on Wed Nov 19 01:07:22 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Fred G on Wed Nov 19 00:15:51 2014. That survey was taken before the new open enrollment began for this year. Why don't we wait until the new realities of ACA set in before we start banging the pots together. |
|
| (1241352) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Olog-hai on Wed Nov 19 02:41:19 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Train Dude on Wed Nov 19 00:03:49 2014. Never mind said resentment increasing when certain liars are caught in lies and refuse to apologize. |
|
| (1241353) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Olog-hai on Wed Nov 19 02:41:50 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Train Dude on Wed Nov 19 01:07:22 2014. Sure, so we can see them fall to 3 percent. |
|
| (1241359) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Fred G on Wed Nov 19 06:37:55 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Train Dude on Wed Nov 19 01:07:22 2014. Speaking of reality, a poll taken of those that are insured is more realistic than one just taken of random people.Your pal, Fred |
|
| (1241363) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by train dude on Wed Nov 19 08:00:11 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Fred G on Wed Nov 19 06:37:55 2014. Thats not responsive to my point. Rates are going up. Deductibles are going up. Both due only to obamacare overreaching. Lets wait for the new data. |
|
| (1241364) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by train dude on Wed Nov 19 08:01:38 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Olog-hai on Wed Nov 19 02:41:19 2014. Liberals will double down on the lies. |
|
| (1241366) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Fred G on Wed Nov 19 08:17:26 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by train dude on Wed Nov 19 08:00:11 2014. It was indeed responsive and a point that needed to be made. We'll see if your predictions come true but the record shows your side has been wrong. My own personal experience contradicts about everything you say.your pal, Fred |
|
| (1241370) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by train dude on Wed Nov 19 08:43:15 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Fred G on Wed Nov 19 08:17:26 2014. Yes because you've gotten yours we can forget those who no longer can afford the coverage they had. |
|
| (1241376) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Fred G on Wed Nov 19 09:09:38 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by train dude on Wed Nov 19 08:43:15 2014. What the fuck are you talking about? I want others to be insured and they are eligible for the same deal I have. In case you don't know the ACA provides for subsidized premiums for those who can't afford insurance. In addition, some states have expanded medicaid to cover uninsured Americans. That's why I support this.If I was a "I got mine so screw you" type, my posts would rhyme with yours. your pal, Fred |
|
| (1241432) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by 3-9 on Wed Nov 19 13:36:25 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Fred G on Wed Nov 19 09:09:38 2014. Please, Fred, you're ruining a good projection moment. :-) |
|
| (1241485) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Train Dude on Wed Nov 19 14:47:52 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Fred G on Wed Nov 19 09:09:38 2014. On the contrary, you said it was working well for YOU. For many Americans, not so much. They can't afford the higher copays. They can't afford the higher deductibles so they have to opt for plans that offer far less than what they had for what they were paying before. I'm sure that they are happy that its working for you. |
|
| (1241488) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by italianstallion on Wed Nov 19 14:49:52 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by Train Dude on Wed Nov 19 14:47:52 2014. "They can't afford the higher copays. They can't afford the higher deductibles so they have to opt for plans that offer far less than what they had for what they were paying before. "These are people who had NO insurance before, so your statement rings hollow. |
|
| (1241493) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by 3-9 on Wed Nov 19 14:53:27 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by italianstallion on Wed Nov 19 14:49:52 2014. Not to mention many "cheap" plans offered below standard coverage.I wonder the states who refused to expand Medicaid coverage have higher rates of disapproval? |
|
| (1241497) | |
Re: ACA approval at 37 percent as new enrollment period commences |
|
|
Posted by Train Dude on Wed Nov 19 14:55:33 2014, in response to Re: ACA approval at 37 percent as new enrollment period commences, posted by italianstallion on Wed Nov 19 14:49:52 2014. Nonsense. Some of my friends can no longer afford the coverage that they had because they are now forced to opt for coverage that they don't needs. |
|
|
Page 23 of 25 |
||